
NYC NYCHHC HIPAA Authorization 2413 2005-2025 free printable template
Show details
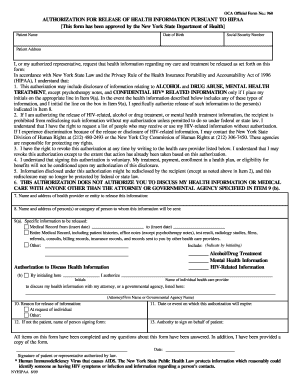
NYC HIPAA Authorization to Disclose Health Information ALL FIELDS MUST BE COMPLETED THIS FORM MAY NOT BE USED FOR RESEARCH OR MARKETING, FUNDRAISING OR PUBLIC RELATIONS AUTHORIZATIONS PATIENT NAME/ADDRESS
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign nychhc hipaa form
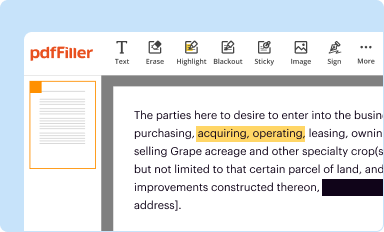
Edit your hipaa authorization fill in form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
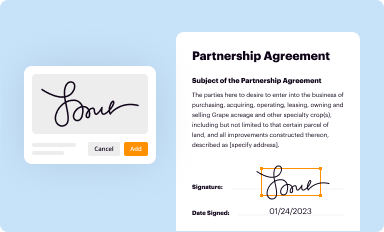
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
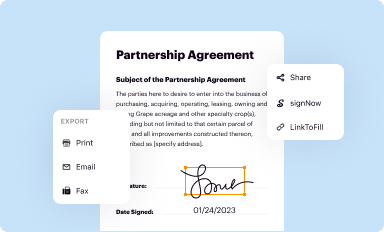
Share your form instantly
Email, fax, or share your hipaa authorization pdf form via URL. You can also download, print, or export forms to your preferred cloud storage service.
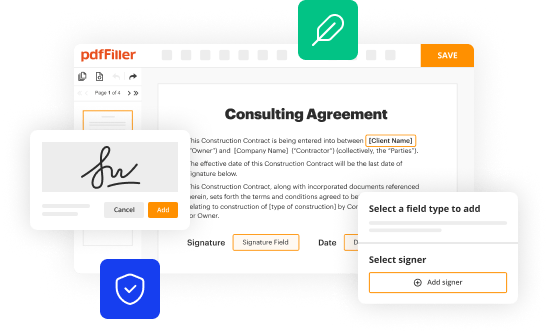
How to edit nychhc hipaa authorization online



To use our professional PDF editor, follow these steps:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit nychhc hipaa form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out hipaa authorization fillable form
How to fill out NYC NYCHHC HIPAA Authorization 2413
01
Obtain the NYC NYCHHC HIPAA Authorization 2413 form from the appropriate source, such as the NYCHHC website or healthcare provider's office.
02
Fill in your personal information at the top of the form, including your name, address, and date of birth.
03
Specify the healthcare organizations that are authorized to disclose your health information.
04
Identify the individual(s) or entity(ies) to whom your health information will be released.
05
Clearly state the purpose of the disclosure, such as for treatment, payment, or healthcare operations.
06
Indicate the types of information that will be released, whether it's specific medical records or all health information.
07
Sign and date the form to authenticate your request.
08
Provide a copy of the completed form to the healthcare provider while keeping one for your records.
Who needs NYC NYCHHC HIPAA Authorization 2413?
01
Patients who wish to allow their healthcare providers to share their medical information with other providers or entities.
02
Individuals needing to grant access to their health records for family members or caregivers.
03
Anyone requiring the release of medical information for insurance claims or legal purposes.
Fill
hhc hipaa form
: Try Risk Free
People Also Ask about hipaa authorization online
How do I make an authorization form?
Things You Should Know Complete the letter's heading with your name and address, the current date, and the recipient's name and address. Make your letter as concise as possible while providing specific deals for the authorization. Format the document like a business letter and get a witness or notary's signature.
What are the requirements of an authorization?
The core elements of a valid authorization include: A meaningful description of the information to be disclosed. The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
How do I create a Hipaa compliant form?
How to create effective HIPAA compliant forms Using a HIPAA compliant form builder. Collect HIPAA compliant electronic signatures. Collecting all patient information in one intake form. Restricting form field entry. Making form fields required. Using conditional logic in forms. Autocomplete forms.
Can I make Google Forms HIPAA compliant?
Are Google Forms HIPAA compliant? Standard Google Forms are not HIPAA compliant. However, you can make them HIPAA compliant by signing a business associate agreement with Google along with changing security and privacy settings on the account to safeguard protected health information (PHI) and other sensitive data.
How do I fill out my authorization?
What are the details to be included in an authorization letter? The authorization letter format includes the address and date, salutation, body of the letter with the name and signature of the person you are authorizing, the reason for unavailability, complimentary closing, signature and name of the authorizer.
What is an authorization form used for?
The authorization form (sometimes called a patient HIPAA consent form), essentially serves as a handy dandy permission slip allowing a practice or business associate to use or disclose protected health information (PHI) in the ways a patient wants their data used.
Is Microsoft Forms HIPAA compliant?
Is Microsoft Forms compliant? Microsoft Forms is compliant in the following ways: HIPAA and BAA compliant.
What authorization is required for Hipaa?
The core elements of a valid authorization include: A meaningful description of the information to be disclosed. The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
How do I make an email HIPAA compliant?
To make your email HIPAA compliant there are several things to consider: Ensure you have end-to-end encryption for email. Enter into a business associate agreement with your email provider. Ensure your email is configured correctly. Develop policies on the use of email and train your staff. Ensure all emails are retained.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my hipaa authorization blank in Gmail?
It's easy to use pdfFiller's Gmail add-on to make and edit your nychhc form hipaa and any other documents you get right in your email. You can also eSign them. Take a look at the Google Workspace Marketplace and get pdfFiller for Gmail. Get rid of the time-consuming steps and easily manage your documents and eSignatures with the help of an app.
How can I edit how to hipaa authorization on a smartphone?
The easiest way to edit documents on a mobile device is using pdfFiller’s mobile-native apps for iOS and Android. You can download those from the Apple Store and Google Play, respectively. You can learn more about the apps here. Install and log in to the application to start editing hipaa authorization.
How do I complete nychhc form authorization on an Android device?
Use the pdfFiller app for Android to finish your nychhc form. The application lets you do all the things you need to do with documents, like add, edit, and remove text, sign, annotate, and more. There is nothing else you need except your smartphone and an internet connection to do this.
What is NYC NYCHHC HIPAA Authorization 2413?
NYC NYCHHC HIPAA Authorization 2413 is a legal document that allows healthcare providers within the NYC Health + Hospitals system to disclose a patient's health information to specified individuals or entities in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
Who is required to file NYC NYCHHC HIPAA Authorization 2413?
Patients or their legal representatives are required to file NYC NYCHHC HIPAA Authorization 2413 when they want to authorize the release of their medical records or health information.
How to fill out NYC NYCHHC HIPAA Authorization 2413?
To fill out NYC NYCHHC HIPAA Authorization 2413, patients need to provide their personal information, specify the information to be disclosed, identify the recipients of the information, and sign and date the form to ensure it is valid.
What is the purpose of NYC NYCHHC HIPAA Authorization 2413?
The purpose of NYC NYCHHC HIPAA Authorization 2413 is to obtain patient consent for the release of their protected health information, ensuring that such disclosures are made in accordance with privacy regulations.
What information must be reported on NYC NYCHHC HIPAA Authorization 2413?
NYC NYCHHC HIPAA Authorization 2413 must include the patient's name, contact information, the specific information to be disclosed, the purpose of the disclosure, names of recipients, and the patient's signature along with the date.
Fill out your NYC NYCHHC HIPAA Authorization 2413 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Records Additional is not the form you're looking for?Search for another form here.
Keywords relevant to hipaa authorization form
Related to hipaa authorization printable




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
